Subcutaneous vs Intramuscular Testosterone: What the UK Evidence Says
What the published TRT trials and UK guidelines actually say about subcutaneous vs intramuscular testosterone, and where 29G shallow SC fits alongside traditional IM.
By Daisy Lin
Medical Writer • Reviewed April 25, 2026
For testosterone replacement therapy, the published evidence shows subcutaneous administration of testosterone esters produces equivalent serum levels to intramuscular at the same dose, with lower self-reported pain and higher patient preference. SC is off-label in the UK regulatory sense — no UK-licensed testosterone product is approved for the SC route — but the Endocrine Society guidelines and the Spratt 2017 trial support it as an evidence-based alternative for cypionate and enanthate. Nebido (testosterone undecanoate) remains IM-only because its depot mechanism depends on muscle vascularity.
The UK testosterone replacement therapy (TRT) landscape has changed materially in the last five years. Subcutaneous administration of testosterone esters — historically considered an off-label workaround, primarily by people transitioning gender — now sits alongside intramuscular injection as an evidence-supported route. The licensed indications have not caught up, but the clinical evidence has.
This article covers what the published trials and clinical guidelines actually say, what the route choice changes for the patient, and where 29G shallow subcutaneous fits. It is not dosing advice. It is not a recommendation that any reader change their administration route. It is a literature summary so that conversations with your endocrinologist or TRT clinic are better informed.
What's licensed in the UK
Three injectable testosterone preparations are commonly prescribed in the UK:
- Nebido (testosterone undecanoate) — long-acting depot, licensed strictly for deep intramuscular injection every 10–14 weeks. The SmPC is unambiguous on the route.
- Sustanon 250 (testosterone esters: propionate, phenylpropionate, isocaproate, decanoate) — mixed-ester preparation, licensed for deep IM injection every 2–3 weeks.
- Testosterone cypionate / enanthate (single-ester preparations, often imported or compounded) — licensed for IM injection in most jurisdictions.
There is no UK-licensed testosterone product approved for subcutaneous administration. SC use of testosterone cypionate or enanthate is therefore "off-label" in the regulatory sense — the product is being used outside the licensed indication. In UK clinical practice, off-label use is permitted where there is a clinical rationale and patient consent; the GMC's guidance on prescribing off-label is the governing framework.
What the published evidence actually shows
The pivotal study is Spratt et al. 2017 in J Clin Endocrinol Metab, which compared subcutaneous testosterone cypionate (or enanthate) administration to traditional IM injection in transgender male patients (n=63). Outcomes:
- Equivalent serum testosterone levels at the same dose, with subcutaneous showing slightly more stable trough-to-peak ratios
- Lower self-reported pain during and after injection
- Higher patient preference for subcutaneous administration (around 80% of participants preferring SC after experiencing both)
- No significant difference in adverse events
The Wilson et al. 2018 observational study in Annals of Pharmacotherapy reviewed real-world subcutaneous testosterone use across a larger cohort and reached similar conclusions: serum levels are achievable and stable, patient experience is more favourable than IM, and no new safety signals emerged.
The Endocrine Society 2018 Clinical Practice Guideline on testosterone therapy explicitly mentions subcutaneous as an acceptable alternative route, while noting the licensed-indication caveat. The British Society for Sexual Medicine guidance is more conservative, deferring to the licensed IM route.
What the route change means for the patient
Needle gauge and length
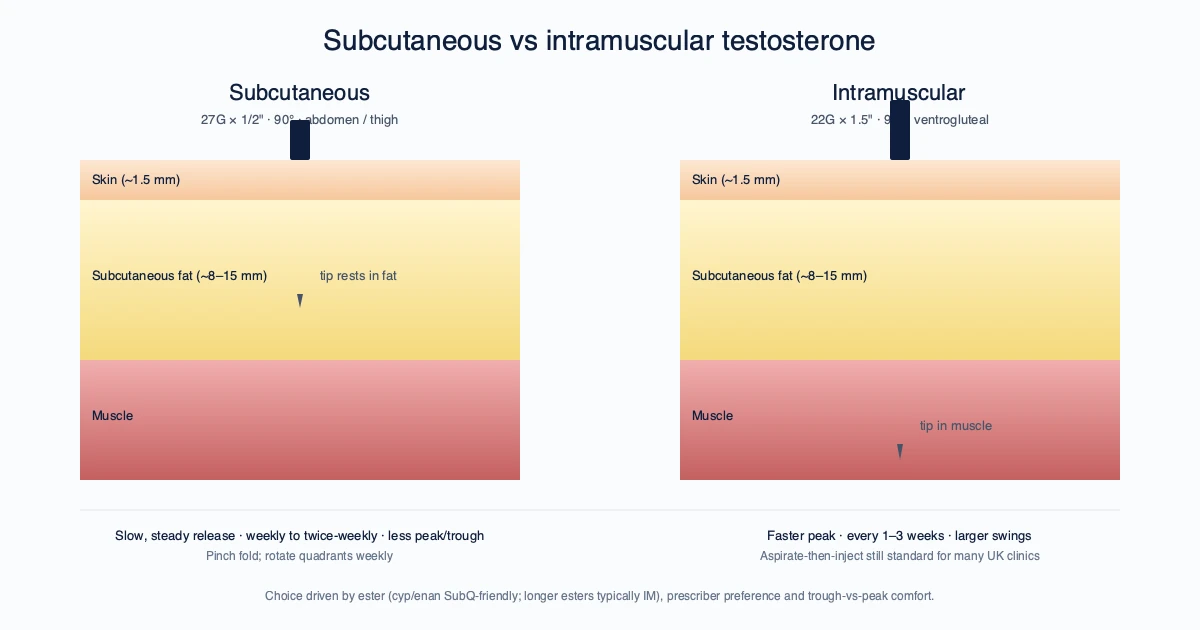
IM testosterone administration in the UK is typically performed with a 23G or 25G × 1.5 inch (38 mm) needle, drawn up through an 18G or 21G drawing needle. The length is necessary to reach the vastus lateralis or gluteal muscle in adults; the gauge accommodates the viscosity of oil-based testosterone preparations.
Subcutaneous administration uses a 27G or 29G × 1/2 inch (12.7 mm) insulin-style syringe. The shorter length cannot reach muscle through the abdominal subcutaneous fat layer in essentially any adult, which is the entire point — the dose stays where it is intended.
The volume difference is also relevant. IM injection of 1 mL of oil-based testosterone is routine; SC injection volumes are typically capped at 0.5 mL per site to avoid pressure-driven discomfort, with larger doses split across two sites or two injections.
For the SC route, the InjectKit 29G × 1/2 inch insulin syringe 100-pack is the syringe most prescribers in this space specify, paired with a separate 21G or 22G drawing-up needle for the oil.
Injection frequency
Pharmacokinetic studies suggest that subcutaneous administration produces a slightly more sustained release profile than IM with the same ester at the same dose. In practice this often translates to switching from once-every-two-weeks IM to twice-weekly SC at correspondingly lower per-injection doses, producing flatter testosterone levels with less week-to-week variability.
This is a clinical decision, not a patient decision. The dose calculation requires your prescriber.
Pain and tissue trauma
The Spratt et al. data on pain reporting is consistent with what mechanical considerations would predict: a 29G needle through 12 mm of tissue is meaningfully less traumatic than a 23G needle through 38 mm of tissue. Reduced pain matters at every-three-day or twice-weekly dosing — IM injection is tolerable at every-two-week intervals but harder at higher frequencies.
Where IM is still the right choice
The route change is not universal. The cases where IM remains preferred:
- Nebido (testosterone undecanoate) is licensed only for IM and the depot mechanism depends on muscle vascularity. Do not attempt SC administration of Nebido — there is no evidence base, and the long-acting depot pharmacokinetics may not behave as expected.
- Patients on stable IM regimens with good levels and no injection-related distress have no reason to change. The evidence supports SC as an alternative, not a replacement.
- Patients who self-inject and find IM more reliable for their hand technique — the deeper, longer needle is more forgiving of small angle variations than a shallow SC injection that needs to clear skin without entering muscle.
Where SC is worth considering
- Patients with frequent IM-related side effects (post-injection pain, bruising, soreness lasting days)
- Patients on every-two-week IM where peak/trough swings are bothersome — switching to twice-weekly SC at a lower per-dose can flatten the profile
- Patients with limited mobility or hand strength who find IM injection in the gluteal or quadriceps difficult; abdominal SC is much easier to self-administer
- Female-dose testosterone (off-label, post-menopausal) — the very small dose volumes (0.05–0.1 mL) are easier to measure and inject SC with a 1 mL insulin syringe than to dilute and IM
A note on equipment
For those whose prescriber has agreed to subcutaneous administration:
- Drawing needle: 21G or 22G × 1 inch, for drawing oil from the vial. The wider gauge handles the viscosity. Discard immediately after drawing.
- Injection syringe and needle: 27G or 29G × 1/2 inch insulin-style syringe (1 mL or 0.5 mL barrel depending on dose volume). Single-use, sterile, ISO 7864 compliant. Oil-based esters draw slowly through 29G even when warmed; allow 30–45 seconds for a 0.5 mL draw.
- Alcohol prep pads: standard 70% IPA, individually wrapped.
- Sharps container: home sharps bin. Pen needles cannot go in domestic refuse — UK NHS guidance is clear.
We supply all of the above; the gauge-specific syringes are the reason we run a dedicated 29-g.com content site.
What we are not telling you
We are not telling you a dose. We are not telling you a frequency. We are not telling you whether SC or IM is the right route for your testosterone replacement. Those are clinical decisions that depend on your specific prescription, your monitoring data, and your clinician's judgment.
What we are telling you, with citations, is that subcutaneous administration of testosterone esters is an evidence-supported alternative to intramuscular — the literature is clear. If your TRT clinic still defaults to IM only, you can ask why. The answer might be a good clinical one specific to your case. It might also be inertia. The conversation is worth having.
FAQ
Is subcutaneous testosterone as effective as intramuscular? Yes — the Spratt 2017 trial and Wilson 2018 cohort study both showed equivalent serum testosterone levels at the same dose, with patient preference favouring SC.
Can I switch from IM to SC on my own? No. The dose calculation, frequency change and monitoring schedule require your prescriber. SC is off-label in the UK and your clinician needs to agree the route change.
What gauge syringe is used for SC testosterone? Typically 27G or 29G × 1/2 inch insulin-style syringe, drawn through a separate 21G or 22G drawing needle to handle oil viscosity.
Why is Nebido IM-only? Nebido's depot mechanism depends on muscle vascularity for the slow, sustained release profile that gives the every-10-to-14-week interval. SC administration would not produce the same pharmacokinetics.
Does SC testosterone hurt less than IM? Yes — patient-reported pain in the Spratt trial was significantly lower for SC, consistent with the smaller gauge and shorter length.
For 29G × 1/2 inch insulin syringes for shallow subcutaneous injection (single-use sterile, ISO 7864-certified), browse the 29G product range or pick up our own-label 100-pack.
Sources
- Spratt DI, Stewart II, Savage C, et al. Subcutaneous Injection of Testosterone Is an Effective and Preferred Alternative to Intramuscular Injection. J Clin Endocrinol Metab. 2017;102(7):2349–2355 — doi.org
- Bhasin S et al. Testosterone Therapy in Men With Hypogonadism (Endocrine Society Clinical Practice Guideline). J Clin Endocrinol Metab. 2018;103(5):1715–1744 — doi.org
- Bayer plc, Nebido SmPC — emc
- Organon UK, Sustanon 250 SmPC — emc
- Hackett G, Kirby M, Edwards D et al. Adult testosterone deficiency, BSSM statements for UK practice — bssm.org.uk
- Wilson DM, Kiang TKL, Ensom MHH. Subcutaneous testosterone enanthate or cypionate: observational study. Ann Pharmacother. 2018;52(6):549–558 — doi.org
This article is for general information only and is not medical advice. Route-of-administration decisions for testosterone replacement therapy require your prescriber.
Frequently asked questions
Is subcutaneous testosterone as effective as intramuscular? +
Yes — the Spratt 2017 trial and Wilson 2018 cohort study both showed equivalent serum testosterone levels at the same dose, with patient preference favouring SC.
Can I switch from IM to SC on my own? +
No. The dose calculation, frequency change and monitoring schedule require your prescriber. SC is off-label in the UK and your clinician needs to agree the route change.
What gauge syringe is used for SC testosterone? +
Typically 27G or 29G × 1/2 inch insulin-style syringe, drawn through a separate 21G or 22G drawing needle to handle oil viscosity.
Why is Nebido IM-only? +
Nebido's depot mechanism depends on muscle vascularity for the slow, sustained release profile that gives the every-10-to-14-week interval. SC administration would not produce the same pharmacokinetics.
Does SC testosterone hurt less than IM? +
Yes — patient-reported pain in the Spratt trial was significantly lower for SC, consistent with the smaller gauge and shorter length.
For 29G × 1/2 inch insulin syringes for shallow subcutaneous injection (single-use sterile, ISO 7864-certified), browse the 29G product range or pick up our own-label 100-pack.
Related reading
Injecting Thick-Viscosity Medications: a Technique Guide for Oil-Based Injectables
Why oil-based testosterone, Nebido and progesterone-in-oil need different equipment than aqueous injectables, with the warming, drawing and Z-track technique that actually works.
Testosterone for Menopausal Women in the UK: NICE, BMS and the Equipment Question
What NICE NG23 and the BMS Tool for Clinicians say about testosterone replacement for menopausal women, what's licensed in the UK, and the equipment side most articles ignore.
Get your supplies
CE-marked syringes, alcohol prep pads, and bacteriostatic water. Shipped from Spain across the EU and UK.