Testosterone for Menopausal Women in the UK: NICE, BMS and the Equipment Question
What NICE NG23 and the BMS Tool for Clinicians say about testosterone replacement for menopausal women, what's licensed in the UK, and the equipment side most articles ignore.
By Daisy Lin
Medical Writer • Reviewed April 25, 2026
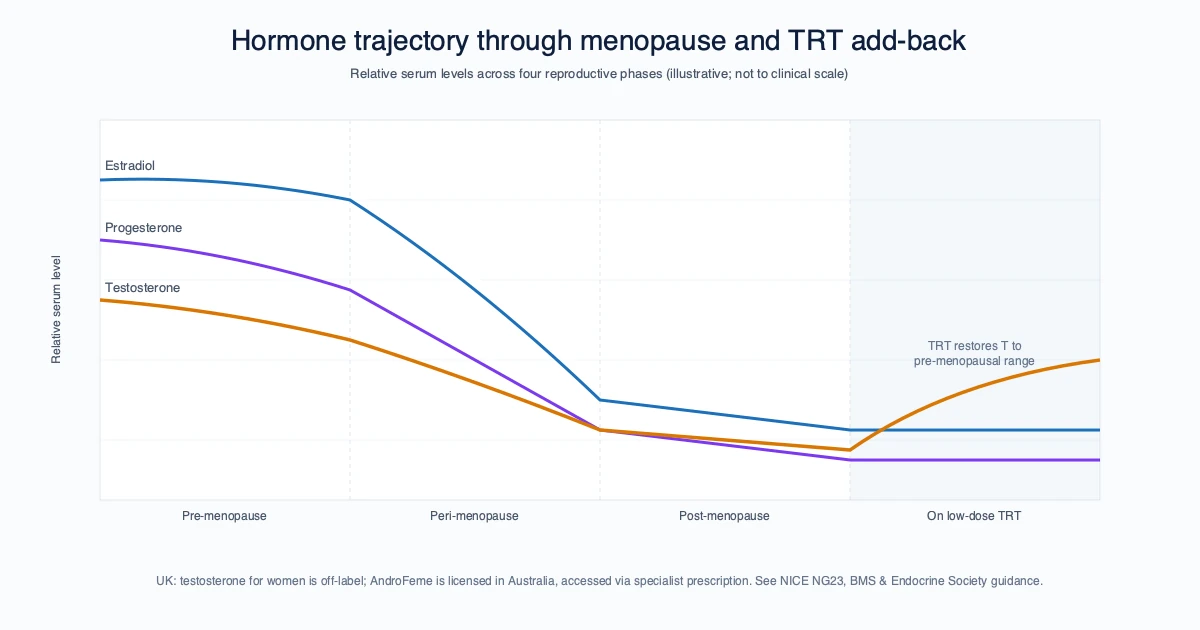
For menopausal women in the UK, testosterone is recommended by NICE NG23 only for low sexual desire that has not responded to standard HRT — not for fatigue, mood or brain fog. The BMS first-line product is AndroFeme 1% cream, available on a named-patient import basis since no UK-licensed female testosterone product exists. Testogel 1% gel is sometimes used off-label at much smaller doses than the male indication. Injectable female-dose testosterone is rare in UK practice because Nebido and Sustanon are formulated for male doses two orders of magnitude larger.
The Menopause Mandate and the post-Davina UK menopause-awareness moment of 2022–2024 has put testosterone replacement therapy for women on the patient agenda at scale. The clinical evidence base for low-dose female testosterone has been building for two decades. The UK regulatory and prescribing landscape has not kept pace. The result is a frustrated patient cohort, a fragmented private-clinic ecosystem, and a great deal of confusion about what is licensed, what is recommended, and what the practical injection equipment actually is.
This article is strictly informational. It does not give dosing guidance. It does not recommend any specific product. It does not advise on whether testosterone replacement is right for your menopause symptoms — that is between you and a prescriber experienced in menopause care.
What NICE NG23 says
The NICE menopause guideline (NG23, updated 2024) addresses testosterone replacement at section 1.4.7:
Consider testosterone supplementation for menopausal women with low sexual desire if HRT alone is not effective.
That single recommendation is the entire NICE position. It establishes that testosterone is appropriate to consider in menopausal women with the specific indication of low sexual desire that has not responded to standard HRT. It does not specify a product, a dose, a route, or a monitoring schedule. NICE leaves those operational details to the British Menopause Society and individual prescribers.
The recommendation is also narrowly scoped. NICE does not currently recommend testosterone for fatigue, mood, brain fog, energy or any of the wider symptom set the patient community most often associates with low testosterone. The guideline is explicit on this point — sexual desire is the only NICE-supported indication.
What the BMS Tool for Clinicians adds
The British Menopause Society Tool for Clinicians is the operational document UK menopause specialists work from. It expands on the NICE recommendation with specifics:
- Indication: low sexual desire (Hypoactive Sexual Desire Dysfunction) in menopausal women on adequate systemic HRT
- First-line product: AndroFeme 1% testosterone cream, licensed in Australia, available in the UK on a named-patient import basis
- Off-label option: Testogel (testosterone 1% gel licensed for male hypogonadism), used in much smaller doses than the male indication
- Dose range: low-dose, with the BMS document providing the specific micro-dose figures that we are not reproducing here
- Monitoring: serum total testosterone via blood tests, with specified target ranges
- Duration: typically 3–6 month trials with reassessment
The BMS Tool is the document any UK menopause-experienced GP or specialist will reference. It is also the document private menopause clinics typically work from. Reading it is worthwhile for any patient who wants to understand what their prescriber is following.
What's actually licensed in the UK
| Product | Type | UK status | Indication |
|---|---|---|---|
| AndroFeme 1 | Testosterone 1% cream | Not licensed in UK; named-patient import | Australian-licensed for female low sexual desire |
| Testogel | Testosterone 1% gel | Licensed | Male hypogonadism only, off-label for female use |
| Tostran | Testosterone 2% gel | Licensed | Male hypogonadism only, off-label for female use |
| Nebido | Testosterone undecanoate IM | Licensed | Male hypogonadism only, generally not used for female TRT due to dose magnitude |
| Sustanon 250 | Testosterone esters IM | Licensed | Male hypogonadism only, generally not used for female TRT |
The honest summary: there is no UK-licensed testosterone product approved for female use. AndroFeme is the BMS-recommended first-line, and it is available only on a named-patient import basis, which means each prescription requires the prescriber to import the product specifically for the patient. This is administratively burdensome and means many UK NHS providers will not prescribe it, referring patients to private menopause clinics instead.
Why injectable female testosterone is rare in the UK
The two licensed UK injectable testosterone preparations (Nebido, Sustanon) are designed for male replacement doses — Nebido at 1000 mg every 10–14 weeks, Sustanon at 250 mg every 2–3 weeks. Female testosterone replacement is two orders of magnitude smaller: typical female doses are in the low single milligrams per week range, not hundreds.
Diluting Nebido or Sustanon to deliver a female-dose volume produces measurement challenges, and neither product is licensed or formulated for that use. The dominant route in UK menopause practice is therefore transdermal — AndroFeme cream or Testogel gel, not injection.
There is a small private-clinic and self-prescribing community that uses diluted testosterone cypionate or enanthate by subcutaneous injection at female doses (typically 1–2 mg twice weekly, drawn into a 1 mL or 0.3 mL insulin-style syringe). This is genuinely off-label and operates outside the BMS recommendations. It is also a practice that does occur in the UK, by clinicians and patients who have considered the trade-offs.
The equipment question — what gauge, what length, what syringe — is the part we are qualified to address. The clinical decision is not.
The equipment side
For female-dose testosterone administered by subcutaneous injection (which is the off-label, private-clinic-supervised route, not the BMS first-line):
- Syringe: 1 mL or 0.3 mL insulin-style syringe with integrated needle. The 0.3 mL syringe with finer graduations (every 0.5 unit on a 100-unit scale = 0.005 mL) is preferred for very small doses where measurement precision matters.
- Gauge: 29G or 30G × 1/2 inch is standard for shallow subcutaneous injection of low-volume oil-based testosterone.
- Drawing: a separate 21G or 22G drawing-up needle is recommended to handle the oil viscosity. Drawing through a 29G is impractical.
- Site: abdominal subcutaneous, with the same rotation rules as any other subcutaneous injection.
- Volume: typically capped at 0.2 mL per injection site to avoid pressure-driven discomfort.
We supply the equipment. We do not supply the medication, do not advise on prescription routes, and do not recommend the off-label private-clinic pathway over the BMS-recommended cream pathway. Both have their place. Your prescriber and your menopause specialist are the right people to make that decision with.
If your prescriber has settled on SC at female dose, the InjectKit 29G × 1/2 inch insulin syringe 100-pack is the syringe-and-needle combination the equipment list above describes. For reconstitution of certain compounded oil-or-aqueous preparations, the 30 mL bacteriostatic water vial is the matching diluent.
Common questions
Why won't my GP prescribe testosterone? The most common reason is that AndroFeme requires named-patient import, which is administratively unfamiliar in primary care. Testogel/Tostran prescribed off-label for female use is a clinical judgment call that many GPs decline to make without explicit menopause specialist support. Referral to an NHS menopause clinic, where they exist and have capacity, is the standard NHS route.
Are private menopause clinics expensive? Initial consultation typically £200–400 in 2026 UK private menopause practice; follow-up visits £100–200; ongoing private prescriptions add medication cost on top. Many patients use private clinics for the testosterone component of their HRT and stay on NHS prescribing for the oestrogen and progesterone components.
Is testosterone replacement safe long-term in women? The Davis et al. 2019 Global Consensus reviewed the evidence available at that point and found no signal of cardiovascular harm, breast cancer increase, or other adverse outcomes at female-dose testosterone replacement. Long-term studies (>5 years) at female doses remain limited, and the BMS Tool is explicit that ongoing monitoring is part of any testosterone replacement.
What about the symptoms NICE doesn't recognise — fatigue, brain fog, mood? The evidence base for testosterone improving these specifically is weaker than for sexual desire, which is why NICE limits its recommendation. Some patients report improvement; some do not. This is one of the areas where the patient experience and the formal evidence base do not yet align cleanly. A trial under specialist supervision with explicit symptom tracking is the constructive route.
FAQ
Is there a licensed female testosterone product in the UK? No. AndroFeme is the BMS-recommended first-line and is available only on named-patient import. All other testosterone products are licensed for male hypogonadism.
Can I get testosterone on the NHS for menopause? Sometimes, via referral to an NHS menopause clinic with capacity to prescribe AndroFeme on named-patient import or Testogel off-label. Many GPs decline to initiate without specialist support.
Why don't menopause specialists use injectable testosterone for women? The licensed UK injectable products (Nebido, Sustanon) are formulated for male doses 100x larger than female replacement doses. Diluting them to female-dose volume is impractical.
What gauge syringe is used for off-label SC female testosterone? 29G or 30G × 1/2 inch insulin-style syringe (1 mL or 0.3 mL barrel), drawn through a separate 21G or 22G drawing needle.
Should I see a private menopause clinic? That depends on whether your NHS provider can offer testosterone within their menopause service. Many patients combine NHS prescribing for oestrogen/progesterone with private testosterone prescribing.
A note on safe practice
If you are using injectable testosterone — by any route, under any prescriber — the equipment standards are the same as for any self-administered injection:
- Single-use needles and syringes only
- Sterile, individually wrapped equipment
- Alcohol pad cleansing of skin and vial top
- Sharps bin for disposal — never household waste
- Storage of medication per the SmPC (refrigerated for vials in most cases)
- Documented dosing — keep a written or app-based log of injection date, site and dose
For 30G × 5 mm and 29G × 1/2 inch insulin syringes for low-volume injection, pick up the 29G × 1/2 inch syringe 100-pack or browse the full 29G product range. The clinical decision belongs upstream of us; the equipment side is where we can help.
Sources
- NICE NG23, Menopause: identification and management — nice.org.uk
- British Menopause Society, Tool for Clinicians: Testosterone Replacement in Menopause — thebms.org.uk
- Davis SR, Baber R, Panay N et al. Global Consensus Position Statement on Testosterone Therapy for Women. Climacteric. 2019;22(5):429–434 — doi.org
- Lawley Pharmaceuticals, AndroFeme 1 SmPC — emc
- Endocrine Society, Testosterone Treatment of Female Sexual Dysfunction — endocrine.org
- Besins Healthcare UK, Testogel SmPC — emc
This article is for general information only and is not medical advice. Testosterone prescribing decisions for menopausal women belong to a menopause-experienced prescriber.
Frequently asked questions
Is there a licensed female testosterone product in the UK? +
No. AndroFeme is the BMS-recommended first-line and is available only on named-patient import. All other testosterone products are licensed for male hypogonadism.
Can I get testosterone on the NHS for menopause? +
Sometimes, via referral to an NHS menopause clinic with capacity to prescribe AndroFeme on named-patient import or Testogel off-label. Many GPs decline to initiate without specialist support.
Why don't menopause specialists use injectable testosterone for women? +
The licensed UK injectable products (Nebido, Sustanon) are formulated for male doses 100x larger than female replacement doses. Diluting them to female-dose volume is impractical.
What gauge syringe is used for off-label SC female testosterone? +
29G or 30G × 1/2 inch insulin-style syringe (1 mL or 0.3 mL barrel), drawn through a separate 21G or 22G drawing needle.
Should I see a private menopause clinic? +
That depends on whether your NHS provider can offer testosterone within their menopause service. Many patients combine NHS prescribing for oestrogen/progesterone with private testosterone prescribing.
Related reading
Injecting Thick-Viscosity Medications: a Technique Guide for Oil-Based Injectables
Why oil-based testosterone, Nebido and progesterone-in-oil need different equipment than aqueous injectables, with the warming, drawing and Z-track technique that actually works.
Subcutaneous vs Intramuscular Testosterone: What the UK Evidence Says
What the published TRT trials and UK guidelines actually say about subcutaneous vs intramuscular testosterone, and where 29G shallow SC fits alongside traditional IM.
Get your supplies
CE-marked syringes, alcohol prep pads, and bacteriostatic water. Shipped from Spain across the EU and UK.